Fractures are one of the most common indications for an imaging examination. However, such evaluation covers a broad range of indications, from initial fracture diagnosis, analysis of fracture fragment displacement and alignment, detection of predisposing lytic lesions, assessment of fracture alignment after closed reduction, assessment of alignment and hardware complications after open reduction, evaluation of potential infection, and assessment of healing. Each radiographic modality, including radiography, computed tomography (CT), magnetic resonance imaging (MRI), and bone scintigraphy has its own unique role in each aspect of fracture assessment.
Imaging Analysis of Diaphyseal Fractures
Fractures are one of the most common indications for an imaging examination. However, such evaluation covers a broad range of indications, from initial fracture diagnosis, analysis of fracture fragment displacement and alignment, detection of predisposing lytic lesions, assessment of fracture alignment after closed reduction, assessment of alignment and hardware complications after open reduction, evaluation of potential infection, and assessment of healing. Each radiographic modality, including radiography, computed tomography (CT), magnetic resonance imaging (MRI), and bone scintigraphy has its own unique role in each aspect of fracture assessment.
Radiography is the mainstay in fracture analysis at any stage. It provides an overall assessment of fracture morphology and provides insight into all potential features of a fracture as it evolves over time. Radiographic analysis requires at least two views for proper assessment, as fractures not seen on one view may be glaringly apparent on another view. Additionally, different views afford different perspectives on fracture analysis, thereby permitting the physician to better detect such complications as displaced fragments, subtle bone destruction, malunion, or hardware failure. However, as radiographic analysis invariably superimposes anatomy in the generation of an image, this modality suffers when more detailed and precise assessment is required.
CT images are acquired by rotating an x-ray tube and an opposing detector quickly around a patient. The x-ray tube is designed to emit a very narrow x-ray beam that passes through the patient and is picked up by the detector. The x-ray beam continuously emits as it encircles the patient and the detector measures differences in x-ray absorption (attenuation). The image is then back computed mathematically. Protocols are designed for specific anatomic locations to maximize image quality and minimize patient dose. Musculoskeletal applications usually use narrower 1 to 3 mm collimation to improve image quality and spatial resolution, especially in small body parts such as the hands or feet. Larger body parts are often scanned with larger collimation of 3 to 5 mm. Once the helical data set is obtained, images can be reconstructed in any plane, usually axial, sagittal, and coronal. Reconstruction parameters significantly influence the final image quality. Finally, filtering algorithms are applied to the data set to maximize resolution of bone or soft tissue depending upon clinical interest. Compared to radiography, CT provides a more detailed and therefore more diagnostically sensitive and specific examination.
Bone scintigraphy is an effective modality in the detection of occult fractures. It is a highly sensitive modality, but lacks specificity. It uses a radioactive isotope that is rapidly taken up into bone that is metabolically active. A normal bone scan virtually eliminates the possibility of fracture. However, a positive bone scan could reflect fracture, infection, tumor, or arthritis. Clinical and radiographic data are used to refine the scintigraphic findings. Additionally, scintigraphy may be used to assess fracture healing since the degree of uptake will diminish over time as bone turnover at a fracture site returns to normal as healing progresses.
MRI also plays an important role in the assessment of fractures. MRI is exquisitely sensitive to the detection of bone marrow edema, an invariable finding in the setting of a fracture. However, MR may not readily differentiate bone contusions from true cortical fractures, especially in the case of avulsion injuries and small chip fractures. These fracture fragments are better delineated with CT. MRI also provides important data concerning concomitant soft tissue injury which is often more important a finding than the fracture itself. In the post-operative setting when metallic hardware is often present to stabilize the fracture, MRI continues to play a role. Use of metal artifact reduction sequences (MARS) significantly limits the distorting effects of metallic hardware on the magnetic field and allows imaging of soft tissues and potential complications in close proximity to hardware.
Operative Treatment of Diaphyseal Fractures
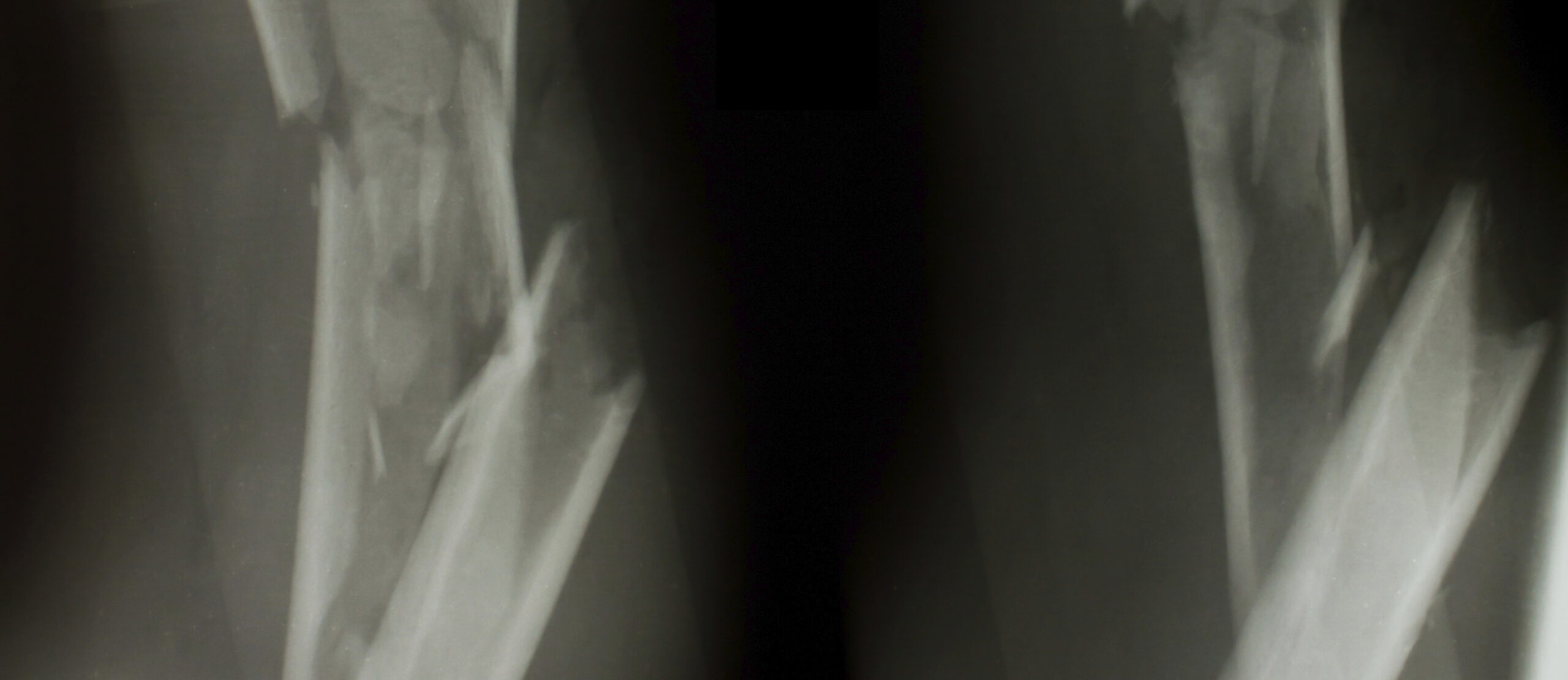
Diaphyseal (long bone) fractures are a common sequellae of traumatic events. These fractures, occurring in the femur, tibia, fibula, humerus, radius, ulna, and long bones of the hands and feet, may be secondary to either direct or indirect forces. Direct trauma often results in open fractures. Indirect rotational forces may result in spiral or spiral wedge diaphyseal fractures with a large surface of bone contact that aids healing. Additionally, these forces often result in less soft tissue and periosteal damage, promoting good healing. Bending forces result in oblique wedge fractures. The degree of trauma in these fractures is usually more significant resulting in a larger amount of damage to soft tissues and periosteum that inhibits healing. Direct forces upon the diaphysis result in a spectrum of fracture patterns including transverse fractures, fragmented wedge fractures, and complex fractures. The forces causing these fractures are often quite large and result in extensive soft tissue damage. These fractures are the most difficult to heal. The determination of fracture type predicts the degree of underlying potential soft tissue damage and provides a guideline for determining the timing of surgery as well as reduction and fixation technique with the ultimate goal of restoration of bone length as well as axial and rotational alignment with respect to the flanking joints.
Diaphyseal fracture fixation is difficult to accomplish using nonoperative means such as plaster casting or traction. Such conservative treatment may result in angular deformity, nonunion, shortening, and stiffness of the adjacent joints. Operative treatment of diaphyseal fractures using either internal or external fixation usually produces better functional results. The goal of fracture fixation is not anatomic reduction and rigid fixation, but rather adequate reduction and stable fixation. Anatomic reduction often leads to excessive periosteal and soft tissue damage while rigid fixation prevents small amounts of motion at the fracture site. Both impair healing and may lead to nonunion.
Operative diaphyseal fracture techniques include intramedullary nailing, plating, and external fixation. Any reduction maneuver should be chosen to both be effective at fracture stabilization and as minimally invasive as possible to preserve blood supply, soft tissue and periosteal integrity. Intramedullary nails are internal splints that bridge a fracture by travelling down the internal shaft of the bone. They allow early weight bearing as well as micro motion at the fracture site, promoting callous formation and bone healing. Distal or proximal interlocking screws are often used to minimize rotational movement. Plating involves the use of fenestrated metal plates and threaded screws for fracture fixation. These are applied to the surface of the shaft of bone and are commonly used when diaphyseal fractures extend into the metaphysis. Often a single interfragmentary lag screw will be placed across the fracture in addition to screws anchoring the stabilizing plate. Conventional plates work by pressing the plate against the surface cortex of bone. This results in crushing of the underlying periosteum and compromising blood supply to the fracture. An improvement over conventional plating, locked compression plates do not compress the bone surface. In these plates, the locking head screws engage the bone and plate separately, providing a space between the plate and the bone while simultaneously stabilizing the fracture. This promotes better healing. Finally, when soft tissue damage is extensive, external fixation techniques may be performed. Because these devices are external, fracture healing may be delayed and there is an increased risk of infection or device loosening. In general, external fixation is a bridge to internal fixation once soft tissue damage has healed.
Summary
Imaging plays a central role in fracture treatment at all stages of the healing process. Radiography provides an overall assessment of fracture morphology and potential complications. CT adds exquisite bone detail, providing detailed assessment of fragment alignment and callous formation to indicate degree of healing. MRI aids in the detection of nondisplaced or incomplete fractures that are not detectable with radiography or CT. Additionally, MRI provides detailed assessment of soft tissues surrounding a fracture that may also guide therapy. Current research revolves around combining novel devices and surgical approaches to further enhance adequate reduction and stable fixation while minimizing invasiveness and tissue damage, thereby leading to a more successful outcome and more rapid and complete return to normal function.
Volume 4, Issue 4: Guidance For Sponsors: Imaging Analysis and Operative Treatment of Diaphyseal Fractures
Originally written by legacy Intrinsic Imaging Medical Director
Contact WCG Imaging to discuss your trial’s imaging needs
We have the team, therapeutic expertise, technology, and ISO-certified quality management systems to provide imaging core lab services to our clients worldwide. Complete the form to get started.